
This post is going to be a bit scattered, there is so much going on that it's exceeded my bandwidth to stay on top of it all. First, I'll give some quick "here's my take" on a bunch of issues, then a random assortment of others with more detail beneath the pictures.
VACCINE ROLL-OUT:
Don't sweat it, we're off to a decent start. If things look shaky a month from now, then pay attention, but this seems mostly consistent with startup bumps on a new and complicated process. As supplies increase and become more predictable, volume will ramp up dramatically and the shelf life in deep freeze is six months. Yes, it could be a lot better, but this is a tiny concern right now.
B.1.1.7 / UK STRAIN:
All new data suggests it is 50-80%ish more transmissible. When it's only 0-10% of total cases it really doesn't affect the curve, but it rapidly becomes 50% then 100% and that's when cases skyrocket. It has taken over SE England, and will be dominant in UK by end of month. UK has gone full national hard lockdown; my guess is that will only be enough to plateau in the SE, maybe not even that and cases will rise during lockdown.
It's a race to get enough vaccines deployed to offset the lift from B.1.1.7; if they can get 30% vaccinated that's about the balance point where vaccine progress equals the force added by B.1.1.7. Deferring second doses is an absolutely necessary part of doing that, no-brainer for their case.
No sign of increase lethality, severity, or any vaccine resistance. Even though the UK is making the right moves, they're starting two months behind. I expect it to get very bad over the next month.
SOUTH AFRICA'S STRAIN:
At the same time, an independent mutant strain from South Africa is getting attention. It seems to be more transmissible than wildtype, but not as extreme (probably?) as B.1.1.7. It has a number of spike mutations that have led to some speculation that it might have some small amount of vaccine resistance, but that looks pretty unlikely. Also, with mRNA vaccines, it's like tweaking a software update to 1.0a if we have to deal with it; a relatively quick/simple process by vaccine standards.
US B.1.1.7 STATUS.
Unlike the UK and Denmark, we have very little sequencing of genomes happening and our processing is laggy, so our picture of current status is almost entirely dark. It has been detected in multiple states, but we don't have enough info to even guess at the prevalence.
It will spread faster than wildtype. It will become our dominant strain. When it does, case counts will explode unless we reach about a 30% vaccination level to counterbalance it. When will it take over? It depends on how far the spread has gone, and we don't have any idea to be honest. A pessimist might conclude March for it taking over, and optimist might expect May, but it should be somewhere in that window...and that's a crazy wide range.
US DISCUSSION ON DELAYED DOSES, HALF-DOSING, ETC
We're in a race to get enough people vaccinated to "flatten" the curve downward before B.1.1.7 takes over and "fattens" the curve upward. Winning means a rapid end to the pandemic, minimized deaths, and a fairly quick return to the new normal. Losing means...well, watch the UK over the next 6 weeks.
If we were at all sure that the 2-dose vaccine rollout will be far enough along to squash the B.1.1.7 rampup, there'd be much less need to consider more aggressive vaccine strategies. But we don't know how many vaccines we'll have per month, how well we'll be able to deliver them, how much B.1.1.7 we have, or when it will take over.
With all that uncertainty, there is a very high quality debate going on about doing one dose for twice as many people (which appears to provide about 90% protection for at least six weeks with no hint of fade), which could end the pandemic faster, save lives, and eliminate the chance of B.1.1.7 blowing everything up.
On the other hand, there are scientifically valid concerns. The second dose is probably needed at some point to get long-term immunity. We don't know if delaying can compromise that, or how long we could delay before we lose some of the long-term benefit. Valid points, and it's a situation of estimating the risks of slower rollouts vs. the risk of unintended consequences. Not an easy call; I lean toward doing 1-dose for at least the first 2-3 months, but I could be convinced otherwise.
There's a similar suggestion to do two half-doses on the original schedule. Instead of 100 micrograms plus 100 more 21 or 28 days later, this would be 50 micrograms plus 50 more at 21 or 28 days. It turns out that the studies showed the half-dose gave similar immune reactions, but there's uncertainty with this approach as well.
Note that if the vaccine rollout is slower than we expect, that strengthens the argument for deferring or half-dosing, because delay gives B.1.1.7 extra time. A very fast and smooth rollout weakens the argument for changing the protocol.
CURRENT STATE OF THE PANDEMIC IN THE US:
Case counts and death reports are still bouncing from holiday and weekend effects, I'm ignoring them. Hospitalizations continue to rise, especially in the south, and are at weirdly similar levels now (with different directions) in the four regions...but hospitalizations is a lagging indicator.
I'm basically ignoring case numbers now, because we should be getting an overshoot as delayed reporting catches up from the holidays - so we had an illusion of slowing and now an illusion of accelerating. My guess is that, taken together, the Wed and Thu evening updates should be the first ones to give us a read on where we're really at. My expectation is that we've plateaued or started down, but that's mostly a guess.

This first pair of graphs was from Andy Slavitt's tweet linked above.
I don't know the source, but the presentation is brilliant for understanding what B.1.1.7 means in the US. These graphs are models of what we could expect for cases and deaths under different starting assumptions for the current prevalence of B.1.1.7 in the US.
CAVEAT: THESE ALL ASSUME A FAIRLY FAST VACCINE ROLLOUT, and it's held constant through all the runs. If we do it faster, all the curves go lower. If we do it later, all the curves go higher, with some well off the top of the chart.
It also assumes that we keep restrictions that are currently enough to hold case counts about level.
If there is almost no B.1.1.7 circulating in the US right now, we're looking at the curves at the bottom. As vaccine penetration increases, fewer people are susceptible, the virus gets fewer targets, and cases and deaths decline. By March 1 we're clearly winning and April 1 is game over.
If we currently have 400-1000 true B.1.1.7 cases (vs. the 3 or so we've ID'd), you get the yellow or red curves. (If I had to bet, I'd take the red 1000 curve, but that's a huge guess.) Here, the vaccine starts making progress, but as B.1.1.7 becomes a major factor in March, is starts to overrun the vaccine before finally being shut down by continued vaccinations...a close call but no disaster. Also note that the death count never trends back up, presumably due to mostly vaccinating the vulnerable first.
If we're a little bit unlucky and there are already 4000 or 10,000 cases in the US, the vaccine hardly gets onto the playing field before B.1.1.7 explodes the case count. Cases could triple and deaths double from today's high levels.
This is the clearest presentation I've seen on the concepts involved. Remember that this set of charts assumes a competent rollout; if supplies are disrupted or we can't deliver effectively, all the line move up and to the right. Similarly, a deferred-dose strategy could move all the lines lower with the pandemic ending a month or two earlier. Big stakes.
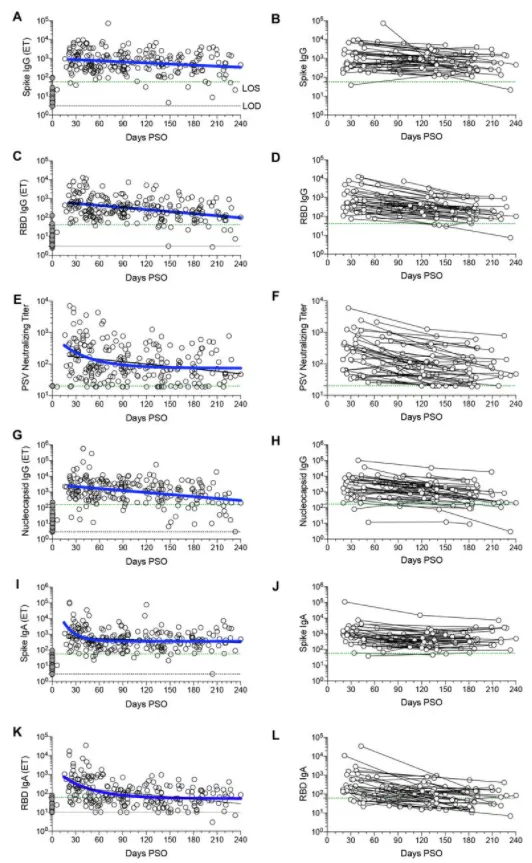
An article with strong evidence that natural COVID immunity is still strong at six months.
There's been a lot of talk in the press that immunity might fade after 3 months, or that it's only good for 3-6 months. Some of that was from early statements that it was clear it lasts at least 3 months.
From what I've read, if there was even a significant decline in immunity by 6 months, we'd be awash in repeat infections. They're still pretty rare.
This is very encouraging news, and bodes well for vaccine effects.

Here's what's happening in the UK, compared to US regions.
The UK is in blue. A week into December, when B.1.1.7 was just reaching dominance in London and SE England, the UK's per capita case counts were relatively flat, and 1/2 to 1/3 the levels in the US regions.
Three weeks later, they've shot up past the US regions, and B.1.1.7 is just now hitting full stride in the rest of the UK.
They've instituted a harsh nation-wide lockdown, which should start to be visible in about 10 days. Until then, expect a rapid rise.
After that...I don't know. I don't think the lockdown will cause a sustained decline. IMO best case is roughly a plateau, and desperate measures to get enough vaccines out to start bending the curve down before lockdown fatigue makes it worse.
I think it's entirely possible that even with a harsh lockdown, numbers will rise. (People are still working, getting groceries, etc., and you know social mixing will still be happening because the Brits have their share of idiots, too.)
Anyway, the UK is going to show us what happens if the vaccine rollout is behind B.1.1.7. It's not going to be pretty.